Written by: Cindy Rikhof
Currently, I am working for almost three years at RRD on the ROBERT-SAS project (Eurostars grant no E113693). Within this project, we investigated the recovery of the lower extremity after a stroke. Now we are running two studies within the project. The first one focuses on the clinical implementation of a robot combined with electrical stimulation, in the (sub)-acute phase after stroke. The second study focuses on the relationship between force and the sit-to-stand transfer and walking after a stroke.
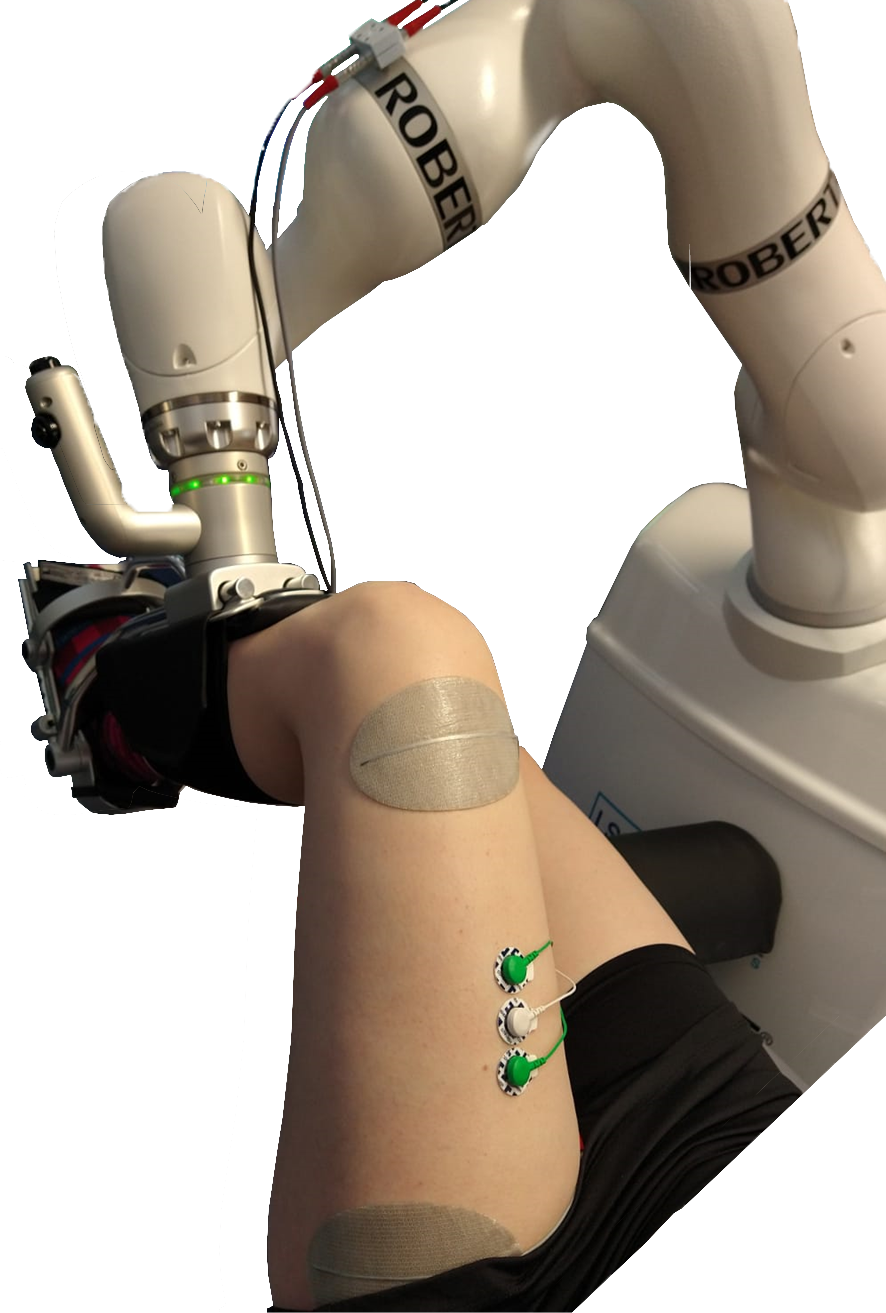
A robot combined with electrical stimulation sounds fancy, but what does it look like? The picture below shows that a brace holds the leg, and the brace is connected to the arm of the robot. With this configuration, the arm can move the leg, on a pre-specified path. The grey pads on the upper part of the leg are for electrical stimulation, which causes muscle contraction and thereby movement. We started with testing in the lab. All participants were comfortable and did not find it tiring. We are currently continuing with the next step: to the clinic!
Clinical pilot
During this clinical pilot, we are investigating the applicability and the early effects of the robot combined with electrical stimulation. The robot is situated in the exercise room of the physiotherapy department at Roessingh, Center for Rehabilitation. We provide training in the early phase after stroke. This training consists of three times a week 30 minutes training for 3-6 weeks. During these trainings, the movements that were frequently practiced are knee extension and ankle dorsiflexion in a lying position. The training sessions are based on ‘Assist-As-Needed’, which means that for every repetition there will be determined which assistance is required to complete the movement. This assistance consists of electrical stimulation and/or mechanical assistance.
Force and sit-to-stand transfer
Does the advantage of having more force in the lower extremity also have an advantage during sit-to-stand and walking? This is the question we are interested in, in this second study. We include both early and late after stroke. The participants are asked to perform some tasks, like knee flexion and extension, ankle dorsiflexion, etc. in a lying position. During these tasks, we measure the force and the muscle activity. The next step in this study is to stand up from a chair and walk in a straight line, again we will measure the muscle activity but also the joint angles.
For this last study, we are still looking for participants! So did you have a stroke or know someone with a stroke in their history with lower extremity problems and does this study sound interesting? Please contact me via: c.rikhof@rrd.nl or +3188-0875742!
If you have any questions regarding this project or my research, please contact me!

Cindy Rikhof
E-mail: c.rikhof@rrd.nl
Tel: 088 087 5742